

It’s a truism: bad health of the population, bad economy. What then is happening globally in the Covid-19 pandemic? When will things return to normal? The pandemic continues to rage in various parts of the world, affecting both developed and emerging markets. On July 7, 2021, The Economist, a magazine that has been running stories on vaccines and the Covid-19 pandemic each week, sponsored a webinar featuring an editor and correspondent on the pandemic beat.
Natasha Lode, health policy editor at the Economist, highlighted some recent issues. She is also host of the Economist’s podcast The Jab, whose tagline reads, “The sharp end of the global vaccination race.” The European Union (EU) has refused to allow the CoviShield vaccine into their vaccine passports. The vaccine was developed in India, using the same technology as another approved vaccine, the AstraZeneca, but the Indian manufacturers neglected to get approval from the EU. Now, India treats it as a national affront. “We need to have the World Health Organization step in,” Lode said.
This may be a foretaste of other disputes about the vaccine, given there are 26 stringent national public health institutes in the world.
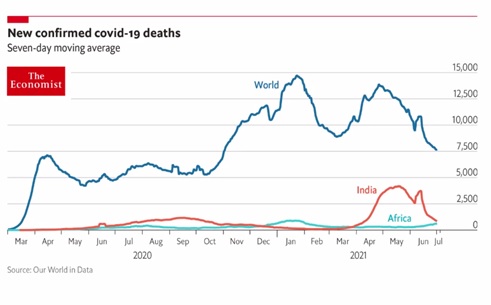
There has been an uptick in the number of world deaths, Lode noted, chiefly due to the Delta variant. India, South America, and the southern states of the U.S.: these are all places where the pandemic is picking up infection and death rates again.
To get a handle on how normalcy is returning to other parts of the world, Lode said there is a “normalcy index” (NI) developed by the Economist. This looks at 8 different variables, such as “time spent outside the home” and “footfall in shops” pre- and post-pandemic. With 100 set as the pre-pandemic NI, the index fell to 40 in March 2020. China and the U.S. are now at 73, the EU is at 71, Britain 62 and India 47.
Lode was interviewed by Alok Jha, science correspondent at the Economist. Jha asked if there was now a “new normal”—whether we would ever go back to 100. There are some notable exceptions. For example, there are 30 percent more planes in the air, compared to 2019, due to physical distancing requirements.
“Nigeria is close to normal,” Lode said, “and the crowds watching tennis at Wimbledon look back to normal.”

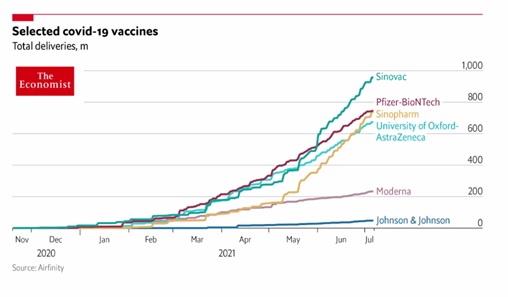
Global vaccine production continues to ramp up. Lode said, “Sinovac production has taken a big jump. We know much less about these vaccines. Possibly it’s the least effective vaccine.”
“The WHO has approved it,” Jha said. “When tested in Brazil, one dose had 50 percent efficacy. It needs to have more trials against the Covid variants.”
Lode and Jha opened the floor to questions from the audience.
Question: how long will immunity last?
“The immune system is very complex,” Lode noted. Preliminary indications from Oxford are that, for the under-70 demographic, “the vaccine might last.” By comparison, SARS immune functions were present in T-cells 8 to 10 years later.
Question: Will we need new vaccines for variants?
“Likely not,” Lode said. In Israel, one study found the Delta variant is very transmissible. “If you want to protect the people you are around, you should still wear a mask.”
“Oxford researchers are looking at changing the vaccine a little,” Lode said. “Once you start producing a variant vaccine, you are competing against the total quantity produced.” She noted they might start to combine two versions of the vaccine in a single jab, “similar to the flu vaccine that contains a combination.”
Question: After receiving the second dose, if a person has more intense side effects, does that mean their immune system is better at fighting Covid?
“The Center for Disease Control website says no,” said Jha, “the side effect intensity does not correlate with efficacy of immune response.”
Question: Regarding vaccine passports, is there a point at which we will have to allow any vaccine?
“Right now, countries can be picky about what vaccines newcomers must have,” Lode said. “But other, bigger players might lean on smaller countries to accept inferior vaccines. I think the passport situation will get really messy.”
Variants of the virus continue to appear. Every time the virus replicates, there is a chance for an error in transcription to occur, and thus a chance at mutation. Some mutations are favorable to the virus, such as making it more transmissible among humans. The alpha variant was identified from U.K.-prevalent strains; the beta variant from South African strains; the delta from India. Very new is the lambda variant, first identified in South America.
“In the hospital, you can watch mutations accumulate,” Lode said. “Evolution in action.”
Question: Is herd immunity basically unreachable?
Jha said, “We don’t seem to know what that level will be. Fauci thinks the level will be 80 percent double-vaccinated.”
“With delta, herd immunity will likely not be possible,” Lode replied.
Question: Could the virus mutate to make the vaccine completely ineffective?
“After 18 months, the worst variant to date is the lambda,” Lode said, “and we don’t have clear evidence whether the vaccine appears to protect against it.” According to a recent World Health Organization (WHO) report, it has been found in 29 countries.
Jha emphasized that the longer the rest of the world is unvaccinated, the more likely mutations will keep occurring, and possibly lead to worse forms.
Question: Should I get a third shot?
“Yes, if you are in the U.K. and it’s available,” said Lode. “Your immunity level may be low and breakthrough infections are possible.” She said that the public health agency is monitoring the situation, “and if they see the number of breakthrough infections is increasing, they will start offering more vaccines.”
Question: Are mRNA vaccines better?
Lode briefly described specific vaccines. The Johnson & Johnson is a viral vector vaccine based on a human adenovirus that has been modified to contain the gene for making the spike protein and requires a single jab. The Pfizer vaccine, an mRNA vaccine, requires a second dose. “There is a lot of mix and match for first and second doses,” Lode said. “In general, heterologous boosting is a good strategy.”
Jha said that both mRNA and adenovirus methods are different ways to stimulate the immune system. “For the Ebola vaccine, the first and second jabs are different. In general, mix and match is good.”
Question: What is the latest news on vaccine-induced immune thrombotic thrombocytopenia (VITT), the clotting disorder attributed to the Astra Zeneca (AZ) vaccine?
“The vaccines are going to millions of people, so even rare problems become very concerning,” Lode said. “Some countries are not giving the AZ vaccine to younger people. They are working on a fix to the vaccine. Johnson & Johnson may be associated with slight clotting. AZ is most popular in low-income countries.”
Question: What about giving the vaccine to children?
“Myocarditis has been observed after some mRNA vaccines are administered, on a level of 56-69 cases per 100,000,” Lode said. “The risk-benefit is still on the side of the vaccine.”
“I’m hesitant to say ‘yes’ to blanket rollout for the 12-17 year old group,” she added. “They are still investigating the 13-year-old who died after the second dose of Pfizer.” ♠️

Notes:
Both graphs are from The Economist.
The Wimbledon 2021 crowd scene is from PA Wire.
The cow cartoon is from Kaiser Health News.
All are permission pending.